Dr. Belal Bin Asaf
Thoracic (Chest) Surgeon
Director, Institute of Chest Surgery,
Chest Onco-Surgery & Lung Transplantation, Medanta Hospital
-
 [email protected]
[email protected]
-
Follow Us:










Dr. Belal Bin Asaf
Thoracic (Chest) Surgeon
Director, Institute of Chest Surgery,
Chest Onco-Surgery & Lung Transplantation, Medanta Hospital


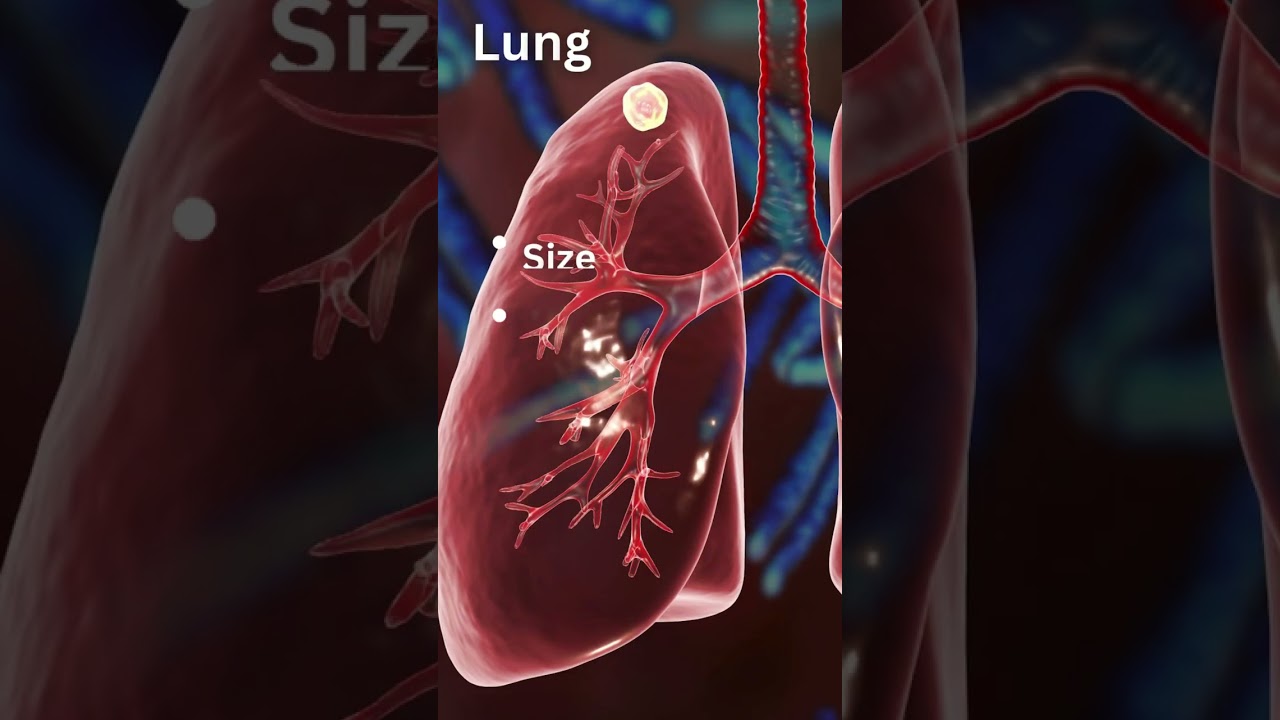
A lung nodule (also called a pulmonary nodule or spot on the lung) is a small, round or oval growth in the lung, usually less than 3 cm in diameter.
Most lung nodules are found incidentally on a chest CT scan done for another reason—such as after a cough, chest pain, or routine health screening.
While the majority of lung nodules are benign (non-cancerous), a proportion can be malignant (cancerous).
Early detection and correct evaluation are crucial for timely and effective treatment.
Key point: Discovering a lung nodule is not automatically a sign of cancer, but it should never be ignored.
Early evaluation helps identify nodules that require only observation versus those needing biopsy or surgical removal..
Lung nodules may arise from a variety of conditions:
Most nodules are silent and found incidentally.
However, some patients—especially with malignant nodules—may notice:
Remember: Symptoms usually appear when nodules are larger or linked to cancer.
CT Scan: First Step
When Observation is Safe
Surveillance Protocol:
When to Intervene
Intervention may be in the form of biopsy or surgical removal.
For Benign Nodules
For Malignant or Suspicious Nodules
Dr Belal Bin Asaf is among India’s leading robotic thoracic surgeons with extensive experience in minimally invasive lung biopsy and cancer surgery.
If you or a loved one has been diagnosed with a lung nodule, do not delay evaluation. Early consultation with a thoracic surgeon can make the difference between simple observation and life-saving intervention.
Book a Consultation with Dr Belal Bin Asaf at Medanta
(In-person and virtual appointments available)
We are here for you! How can we help?

Director
Institute Of Chest Surgery, Chest
Onco-Surgery & Lung Transplantation
Morning: 10:00AM - 2:00PM
Evening 4:00PM - 6:00PM(Mon to Sat)